You are on our international English website. This site features our entire product portfolio worldwide. The products featured may not be available in the US. If you are a citizen from the US, please visit your country website for local information and contacts.
The future, now present, ophthalmic surgical workflow - Brandon Ayres, MD
byZEISS
18 September 202012 minread
COVID-19 as an accelerant to a new model in eyecare
Over the past several years, the healthcare industry has been challenged by a major growth in patients and a smaller number of doctors. The eyecare industry has begun the transition to telemedicine and remote care options to effectively diagnose and treat patients in less time. This enables doctors to diagnose patients remotely, and bring in the patients who require additional treatment or a surgical procedure.
The pandemic was not the cause, merely a catalyst.
With COVID-19, the average ophthalmic surgery model was forced to change dramatically, but the pandemic was not the cause, merely a catalyst. This did not happen overnight: the traditional, doctor-centric and time-intensive exam model has already gradually shifted to a modern exam model that relies more on integrated technologies and less on the ophthalmological exam. However, with new social distancing protocols in place, a contemporary exam model has emerged as a distributed, flexible, and efficient system.
In March 2020, when quarantine measures went into effect in counties across the country, this model had to be drastically reimagined and its development accelerated. As practices reopened, the backlog of patients and lost revenue created a pressing demand to ramp up patient volume swiftly. This required a substantial shift in thinking and practice, and the introduction of new hybrid workflows that utilized the full capabilities of cloud-based surgical planning software like ZEISS VERACITY1 Surgical, which integrates with existing EHRs or management software like FORUM, or FORUM-based surgery planning software like ZEISS EQ Workplace. All create the opportunity to craft a new model of eyecare that offers major benefits for both patients and doctors long-term, especially as patients become accustomed to efficient in-office visits and telehealth consultations.
Brandon Ayres, MD: Practice measures and technology for patient care during the coronavirus pandemic
Third-party Content Blocked
The video player is blocked due to your cookie preferences. To change the settings and play the video, please click the button below and consent to use of "Functional" tracking technologies.
Improving workflow efficiency with process, technology, and people
Like many other eyecare practices, our practice closed down to all but emergency cases extremely quickly – practically overnight. We went from 65 to 70 patients per clinical day to 20 patients per week, or a near 90% drop. It was a sudden, massive shift, not a subtle decline. Our group of doctors and staff suddenly had extra time on our hands to organize the technology we utilized in our practice and update our integrations and workflows so that we could incorporate the devices and equipment to their fullest potential.
When we reopened, our protocols had to take into account the new social distancing measures and patient and doctor safety which – along with the length of time we were closed – meant a full patient load was not immediately possible, and will not be for some time. We had already started moving towards this workflow model; however, we needed to accelerate its development to make it more efficient at every stage.
This new model relies more on technicians for the examination stage and for other non-surgical duties, leaving the doctor open to do things only the doctor can do (evaluation and decision-making). This requires technology that is less user-dependent; it must be fast, simple, and accurate to keep patient time in the office limited.
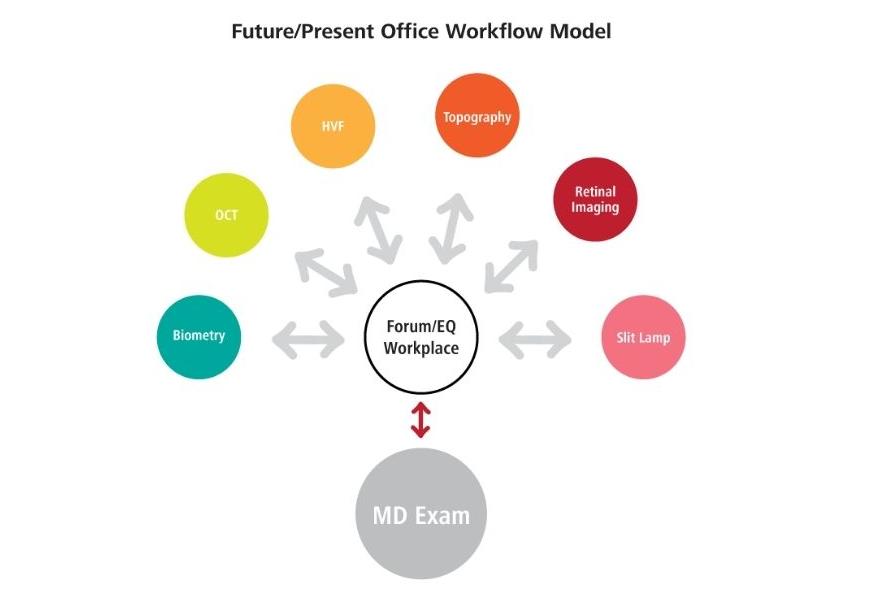
Future / present office workflow model
The future model of eyecare
Increased reliance on technology and technical staff in the office
All data is brought to the doctor using a manageable platform with a friendly GUI
Allows for efficient evaluation of data and surgical/medical planning
More patients can be seen in a shorter amount of time
Allows for remote diagnostics and telemedicine
Office can be used for patient care when doctor is not present
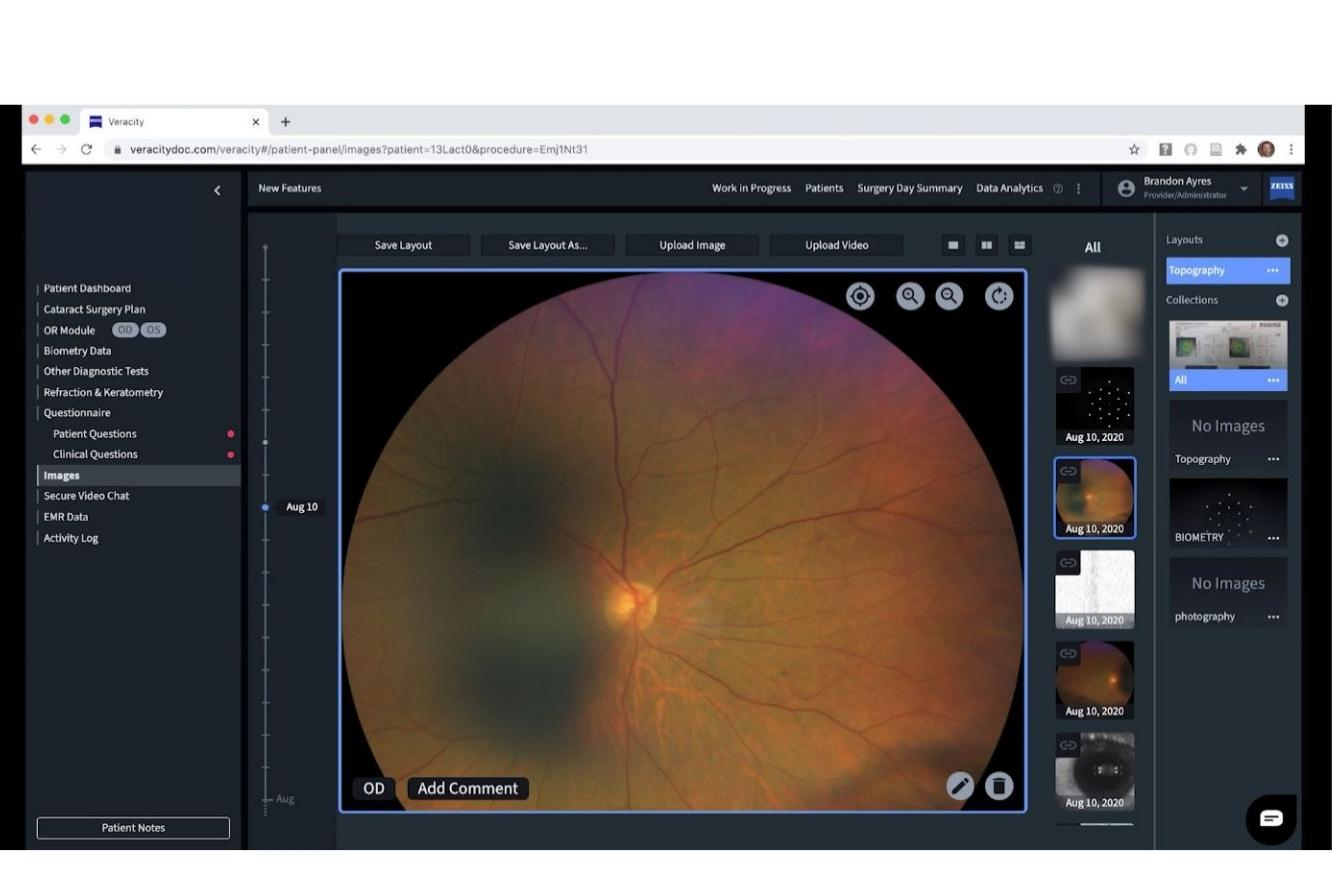
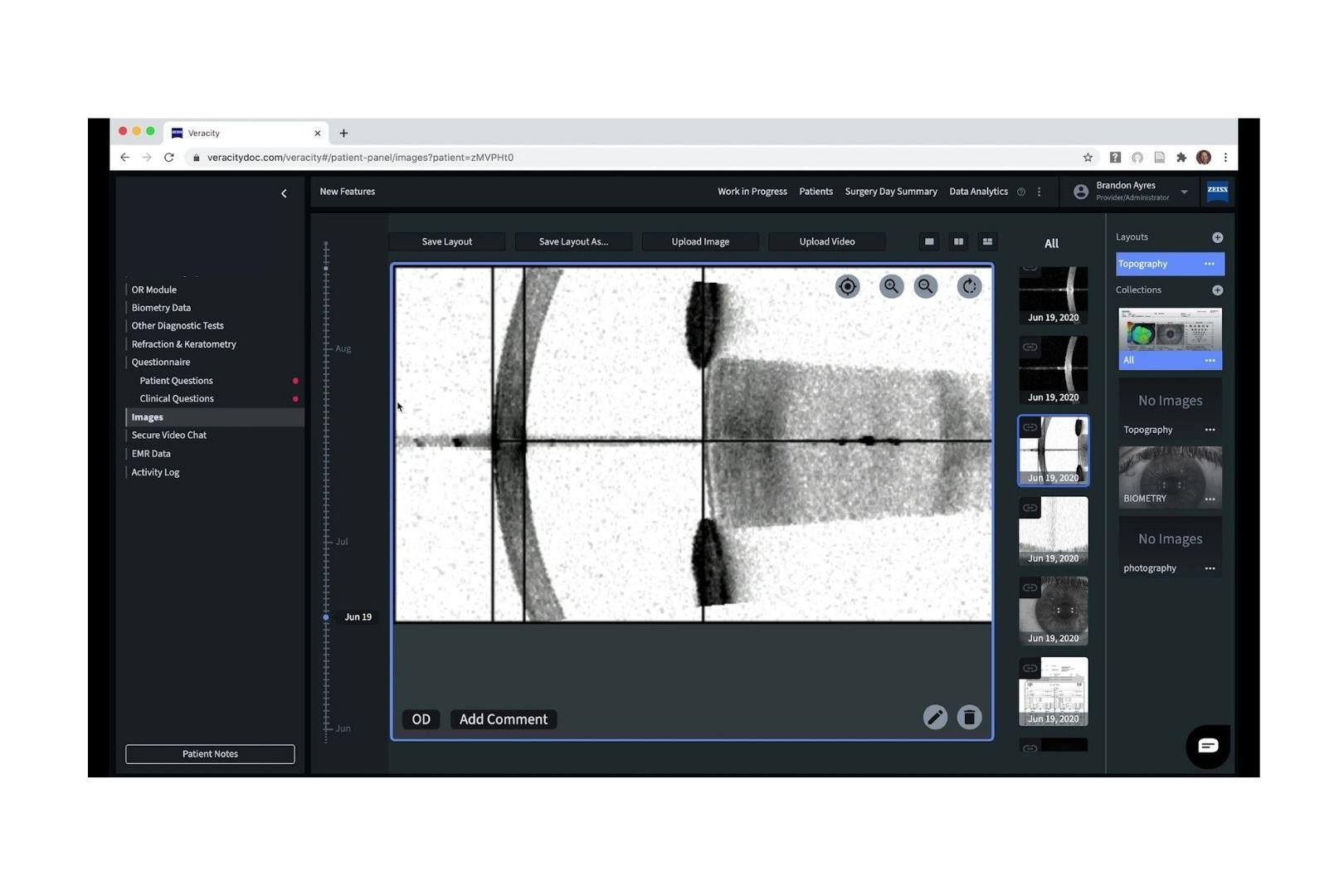
Multiple images are taken in a single appointment and uploaded into VERACITY SURGICAL
Efficiency and flexibility: the twofold benefit of keeping patients out of the office
A 94-year-old female patient presented with signs of glaucoma progression which were substantially advanced from her prior exam six months ago. For several reasons, this patient would be put at risk by coming into the practice for multiple pre-surgical exams: she lived out of town, and between her risk of infection and preexisting conditions, it was in her best interest not to come in for multiple appointments.
So instead of setting multiple appointments for imaging and follow up, we made sure to collect extra images and videos during her primary appointment. That data was uploaded into VERACITY Surgical, and I called a glaucoma specialist to review the imaging. Instead of bringing the patient in for repetitive tests or simply to confirm that we would be scheduling her surgery, we collected the images in a single appointment, and scheduled consultations virtually. Very few surgeons are comfortable with performing surgery on someone they’ve never met; however, we were able to set up a video conference between the patient and the glaucoma specialist to review her exam and schedule her surgery.
Like us, our patients are busy, and they don’t want to come into the office if they don’t have to. This new model allows our patients to take their appointments at home, on their computer or mobile device. Right now, that’s hugely beneficial because it allows them to avoid potential exposure. However, we expect that when given the option, 9 out of 10 of our patients will continue to choose to take their appointments at home. The contemporary model allows patients the benefit of communicating with their doctors one-on-one but in a comfortable environment that saves them time and energy.
Multiple images are taken in a single appointment and uploaded into VERACITY SURGICAL
When coronavirus is no longer a concern for our practice and our patients, we will still have this workflow model in place. Our technicians will still be trained to take full and accurate imaging in a single session, and our doctors will still be comfortable working with patients remotely. While some might always prefer face-to-face interaction no matter what, this workflow will allow for our patients and doctors to choose between the two – and offer quality healthcare no matter what.
We’re learning so much about what we can and should do in medicine. Although we were forced into it by the pandemic, I don’t believe this new hybrid model is going away any time soon. We’re working smarter and more efficiently, and we’re practicing quality medical care: in many ways, it’s improved for both patients and doctors, and the more we explore the possibilities, the better eyecare will become.
As we've put this new workflow into place, we've increased our exam load from 10% to over 70%, without compromising on patient satisfaction or the safety of our patients or our staff.
Download PDF
The future, now present, ophthalmic surgical workflow
Hybrid workflow and digital integration with VERACITY Surgical
Technology and teamwork in the new hybrid workflow
In implementing a hybrid workflow in our office, there were two things that we required from our team: first, a team member to step up as the leader and implementer, and second, for all technicians to feel comfortable with more independence in performing exams on patients. In most cases, that required less training in exam procedures, and more in using the integrations.
As the position of examiner is moving from doctor to technician, it’s crucial that the technology we use is as user-independent as possible. We’re teaching more photography and making sure that our technicians are comfortable with the technology, because we only have one patient visit to capture imaging.
Now that we are trying to do as much as possible digitally or virtually, technicians are receiving training on the integration between our IOLMaster 700, CIRRUS 6000, our Digital Slit Lamp, and VERACITY Surgical which acts as our central database. In many cases, our technicians are already well-trained on taking imaging and performing exams, because we already had the technician-only visits in place for our dry eye patients. The biggest challenge so far has been in training the whole team on the integration with the digital imaging database because it’s based more on knowledge of the software and less on how to use the instruments.
In putting this workflow into practice, one of our team members became an absolutely integral part of the process. For this to work in an office, we had to identify a person who would own the project, and would take responsibility for problem-solving and implementing new ideas and processes. If something isn’t working properly, this person gets in touch with the support teams of the technology we’re using and arranges for a fix. If one of us has a request, they pass that along to the support team, and if that request is urgent, they follow up to make sure it gets resolved.
This person has to be determined, innovative, and willing to take charge and carry a project through to the finish. They become the engineer operating the engine that’s driving the workflow.
ZEISS VERACITY Surgical Integrations in Wills Eye Institute
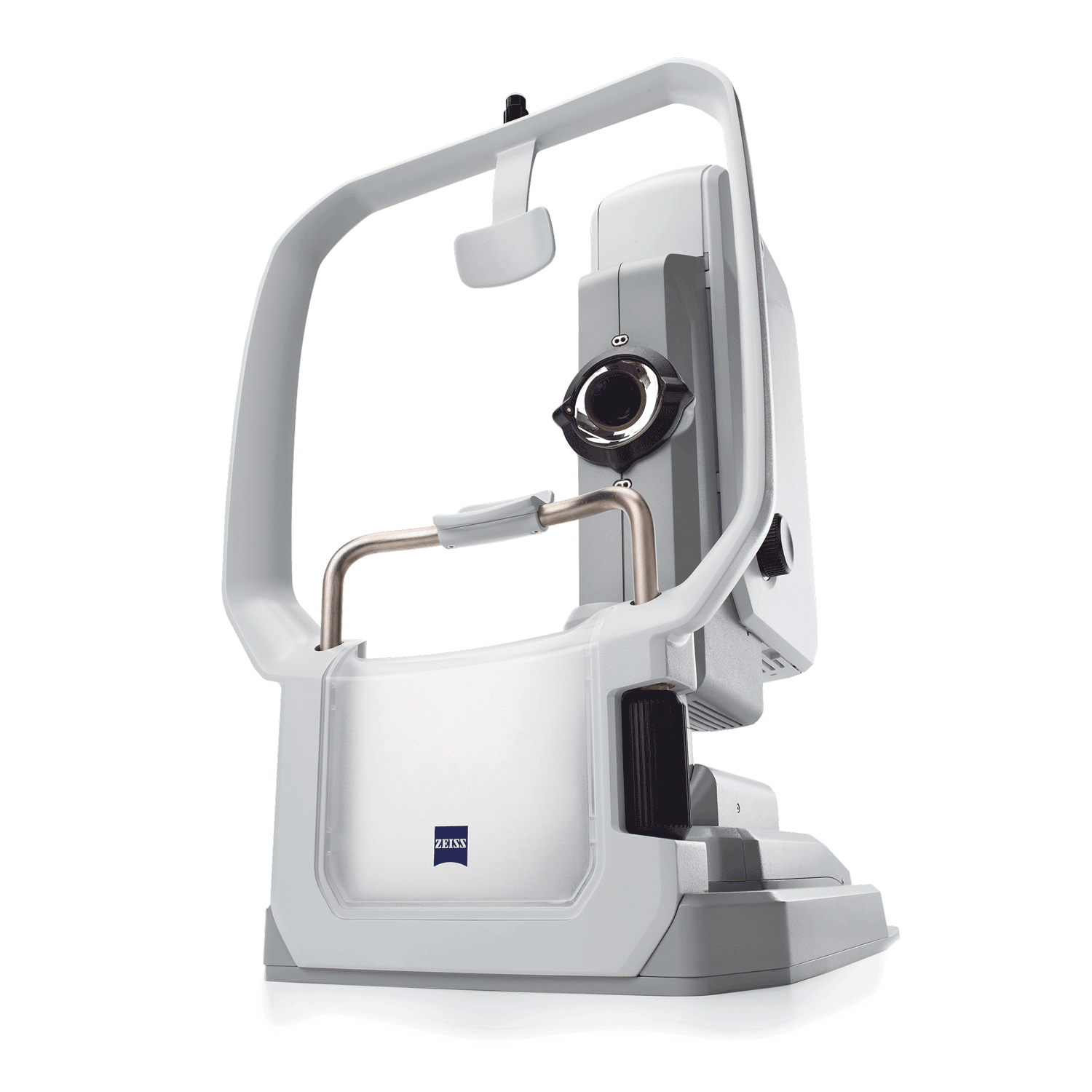
Biometry: IOLMaster 700
● Quick acquisition times
● Total Keratometry
● Foveal alignment
● Works with dense cataracts
● More user independent
● Allows high-quality digital images to be viewed remotely
● Remote consults can be performed without patient return
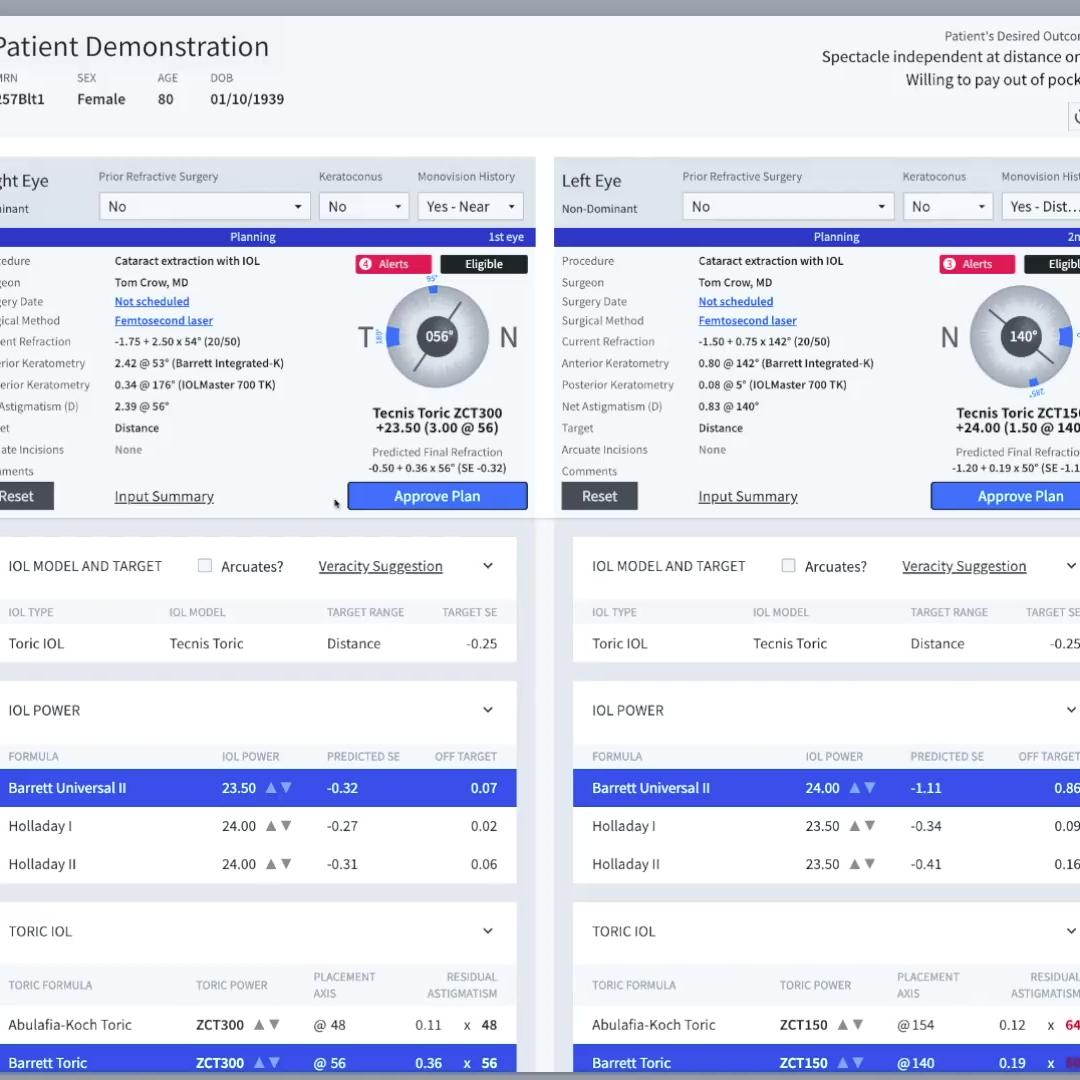
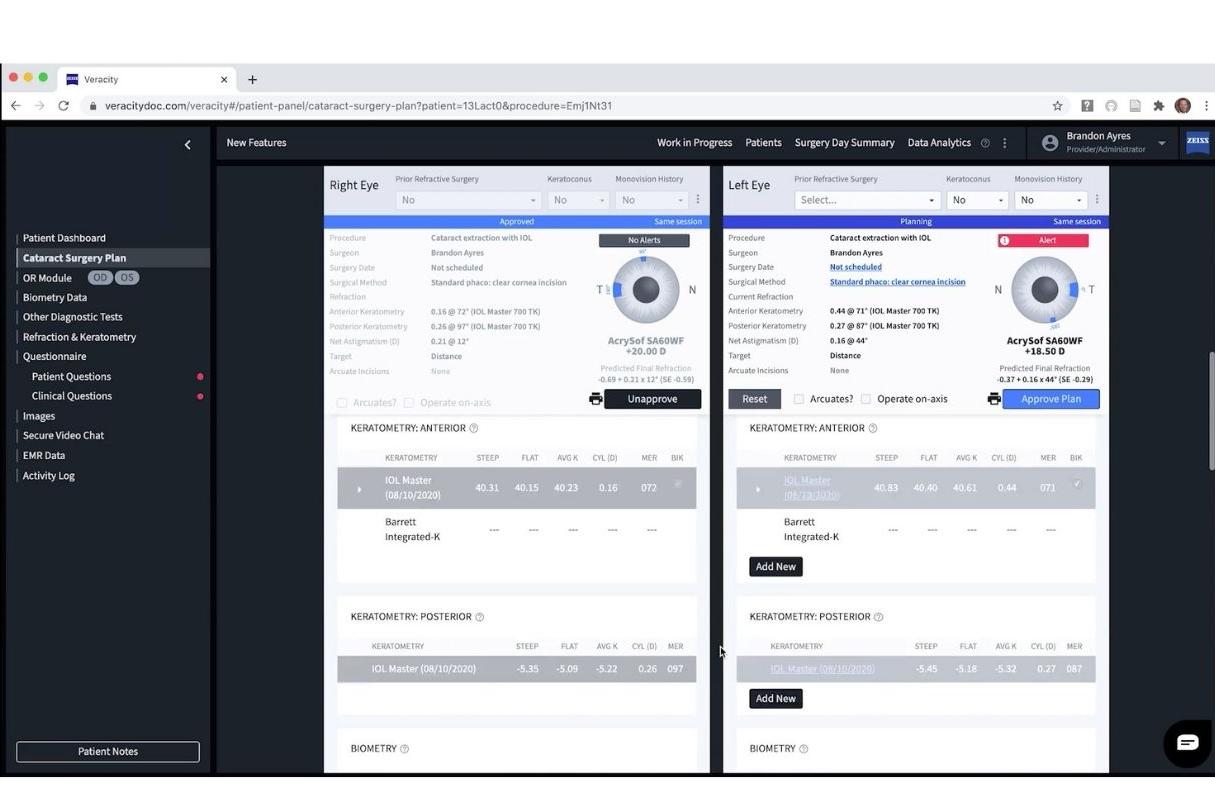
Digital Surgical Planning and Image Viewing: ZEISS VERACITY Surgical
● AI to help with IOL calculation and selection
● Digital Image viewing: OCT, topography, and slit lamp
● Patient communication
● Connects office, OR, patient info, and doctor
● Portable and time-saving
CLARUS Fundus Photography
● Ultra-widefield images visualize the periphery
● Remote image review
By building sustainable hybrid workflows now eyecare practices will be setting themselves up to succeed in the future of eyecare.
ZEISS VERACITY Surgical
Eyecare 3.0: ZEISS VERACITY Surgical and tomorrow
As we continue to develop and expand our practice’s hybrid workflow, we will be working on streamlining and automating the integrations we use so that there is a seamless process between capturing the image on the instrumentation and uploading it to our cloud-based platform.
ZEISS VERACITY Surgical
The next step in this process will be ramping up our patient volume. As we’ve put this new workflow into place, we’ve increased our exam load from 10% to over 70%, without compromising on patient satisfaction or the safety of our patients or our staff. The remaining 30% of our patient volume is likely to be virtual or remote care, even once social distancing protocols are lifted.
This entire hybrid workflow is made possible by the cloud-based platform, which in the case of our practice is ZEISS VERACITY Surgical. By using a digital patient management hub, we’re able to use software as a conduit to get data from the patient to the doctor – and to allow doctors to share patient information when calling for a consult or building a care plan. I think there are quite a few cataract surgeons out there who could increase their surgical volume by using VERACITY Surgical to ensure their surgical workflow is seamless and efficient. Not only will it help increase surgical volume, but it will decrease administrative busy work inside of patient charts.
The pandemic was not the cause of this new model; merely an accelerant. We’ve had the technology that makes this possible for years, and doctors around the world had already begun developing innovative ways to combine and adapt the technology we use to practice with every day. It will be years before people are comfortable in crowds the way we used to be, and even when restrictions are lifted, neither patients nor doctors will want to abandon the accessibility and efficiency of telemedicine. By building sustainable hybrid workflows now, eyecare practices will be setting themselves up to succeed in the future of eyecare. We’re building strategies to meet the upcoming demands: no matter what they are, or when they come.
The author of this article has a contractual or other financial relationship with Carl Zeiss Meditec, Inc. and its affiliates and has received financial support.