Intraoperative radiotherapy (IORT) during surgical resection of glioblastoma
An international pooled analysis of 51 patients


Reading this brief overview does not substitute the reading of the original study, but is just giving an abridged insight and is not necessarily reflecting the opinion of notified bodies and/or regulatory authorities, such as the DQS or FDA.
A brief overview of an international pooled analysis created by Gustavo R. Sarria, MD, on behalf of ZEISS, March 2020.
Original title:
Intraoperative radiotherapy for glioblastoma: an international pooled analysis
Authors:
Gustavo R. Sarria, Elena Sperk, Xiaodi Han, Gustavo J. Sarria, Frederik Wenz, Stefanie Brehmer, Bing Fu, Siming Min, Hongjun Zhang, Shusen Qin, Xiaoguang Qiu, Daniel Hänggi, Yasser Abo-Madyan, David Martinez, Carla Cabrera, Frank A. Giordano
Source:
Sarria GR, Sperk E, Han X, et al. Intraoperative radiotherapy for glioblastoma: an international pooled analysis. Radiother Oncol. 2020;142:162-167. doi:10.1016/j.radonc.2019.09.023
- Local tumor re-growth after surgery is the mostly observed reason for Glioblastoma treatment failures.
- Giving a high intraoperative radiotherapy (IORT) dose during surgery may lead to a prolonged local control rate and survival.
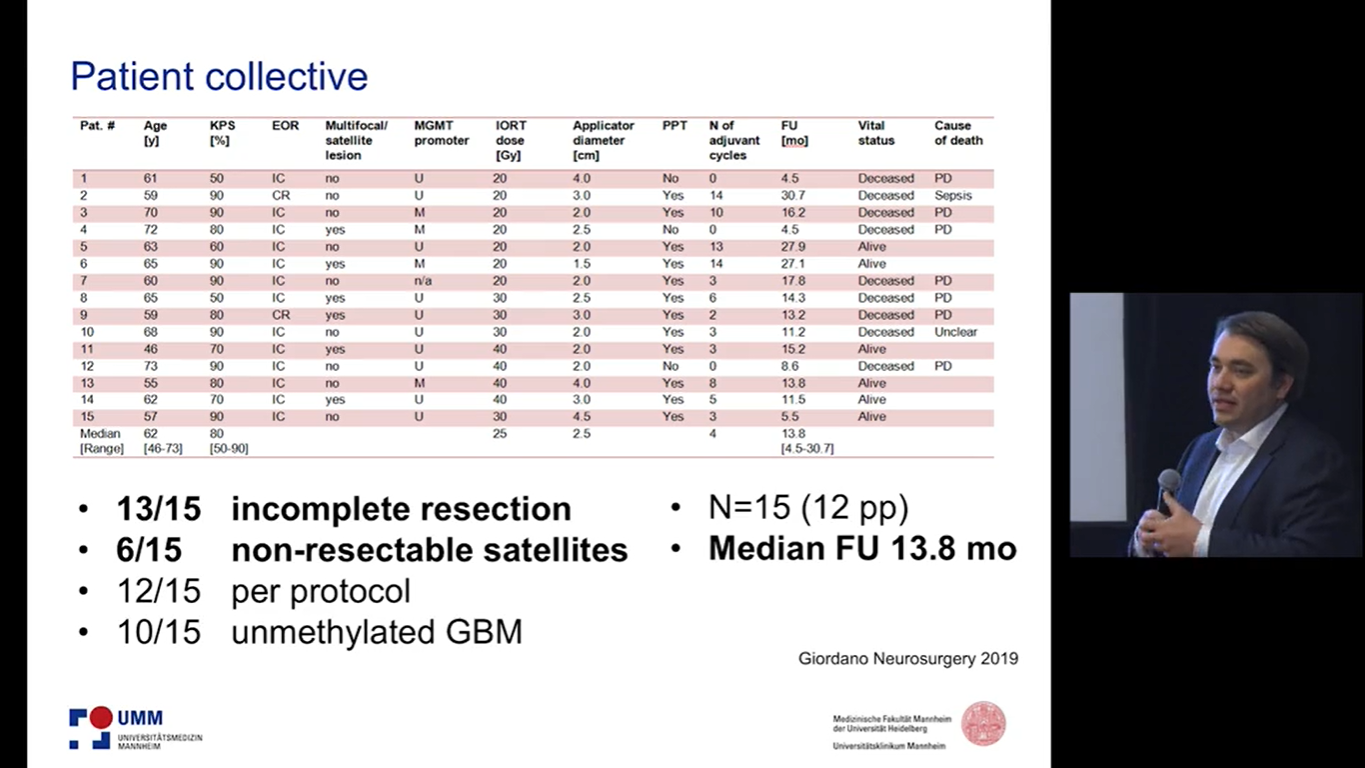
- For this retrospective study, 51 Glioblastoma patients with a median age of 55 were included from five different centers in Peru, China and Germany. Following surgical resection, all patients received IORT with a dose range of 10-40 Gy followed by standard adjuvant radio-chemotherapy and standard chemotherapy.