Improve Your Cataract Practice by Tracking Your Postoperative Outcomes


We, as cataract surgeons, understand in a general sense how often they hit their refractive targets: happy patients return with glowing reports, and less pleased patients volunteer their opinions. However, we know that patient satisfaction does not directly align with the rate at which a surgeon hits his or her refractive targets. Patients who are easily pleased may be just fine with a 0.50 D error, while those with more specific (and perhaps unrealistic) expectations will forever express frustration regardless of the outcome.
Quantitative tracking of personal or practice-wide outcomes offers a data-based counterpart to subjective patient satisfaction. Acquisition of quantitative outcomes data requires a heavy time investment. Further, depending on how data are captured, entered, and organized, each clinic’s dataset may not reflect recent trends or may be insufficiently filterable to answer specific questions.
Rather than manually capture and format my outcomes data, I let ZEISS VERACITY Surgery Planner do the work for me. The process requires no work by myself, the surgeon. As soon as I link my practice’s hardware to the ZEISS VERACITY Surgery Planner, I’m eligible for automated documentation and tracking of patient outcomes. See the article by my colleague Joaquin De Rojas, MD, for more on this topic.
Tracking outcomes patterns doesn’t just satisfy a surgeon’s sense of curiosity. They can improve outcomes on individual technologies, characterize differences among surgical locations, and identify outliers that may inform future cases. All of this works in service of improving surgical success and improving patient results.
Lens-based Analysis
Surgeons who use the ZEISS VERACITY Surgery Planner may track outcomes following the implantation of any particular IOL and may compare outcomes data across multiple IOLs. At the Wolfe Eye Clinic, I review results each quarter to see if any single lens performs distinctly from its counterparts.
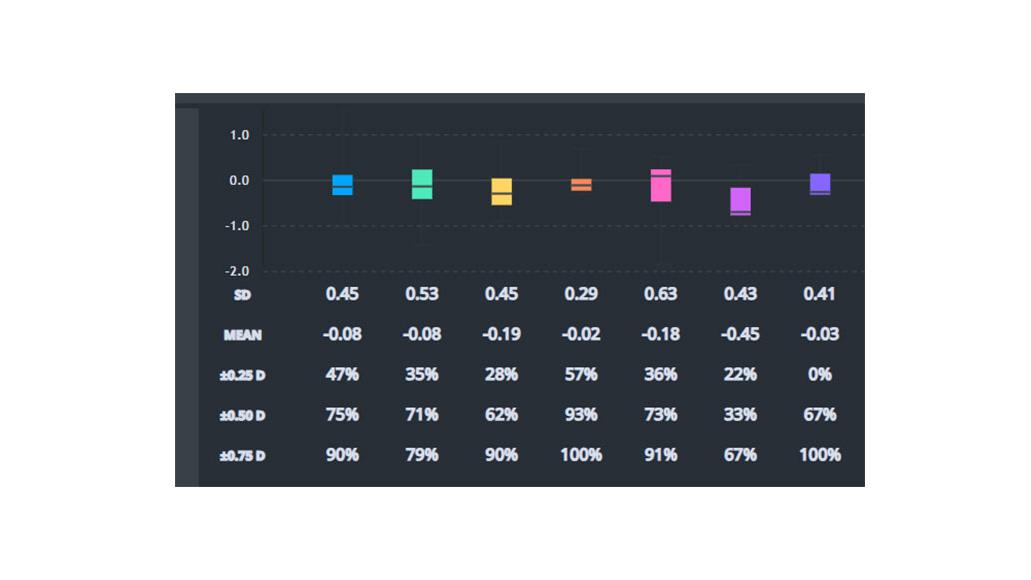
During my most recent analysis of two IOLs—lens X and lens Y—I found the following results:
|
Percentage of Patients Within [____] of Refractive Target
|
|||
|---|---|---|---|
|
Lens |
0.75 D |
0.50 D |
0.25 D |
|
Lens X |
90% |
75% |
47% |
|
Lens Y |
100% |
93% |
57% |
This tells me that while the two lenses perform strongly, Lens Y is slightly better than Lens X at hitting refractive targets.
While some doctors find greater utility in head-to-lens IOL comparisons, others may find more use in comparing classes of IOL technology (e.g., EDOF vs. multifocal IOLs). In particular, this may have value for surgical practices that, after adding a new technology to their offerings, wish to understand how it functions in real-world patients.
Practice Site Analysis
The Wolfe Eye Clinic’s network includes several satellite offices. Presurgical cataract evaluations in our main office use the latest biometric technologies, while evaluations in satellite clinics rely on experienced technicians calculating manual K values.
Unsurprisingly, surgery after manual K calculation results in less precise outcomes than those using captured biometric data from an innovative technology. However, rather than relying on the impression or assumption that outcomes following automated biometric capture are superior to those using manual K measurements, I now can point to data that both underscore and better characterize that claim.
The result? I insist that patients in rural areas who want premium cataract surgery come to our main clinic for presurgical, surgical, and postsurgical care—and I’m confident in that decision because I have the objective data to back it up.
Outlier Analysis
During my quarterly review of outcomes, I always identify and investigate outlier cases. Spotting these cases on a scatter plot of patient outcomes is easy, and the ZEISS VERACITY Surgery Planner interface allows me to hover over or click on any single point on the graph to learn more.
Outlier cases typically still have good outcomes and only present as outliers when viewed within the continuum of cases shown in a given report. The ability to identify these cases and review why they deviated from the mean empowers a surgeon to refine their practice at the margins, giving them the edge to elevate themselves as a surgeon from good to great.

What Comes Next?
Armed with automated, quantitative outcomes data, surgeons can decide how best (if at all) to adjust their surgical approaches for particular patient subtypes or technologies. Note that after you’re comfortable with the process for tracking and analyzing cataract outcomes data, you can also track your refractive surgery outcomes.
Regardless of how you use outcomes data aggregated by the ZEISS VERACITY Surgery Planner, the real story is how the data are collected: in an automated, precise, and organized manner, thereby freeing you from the burden of manual collection and the uncertainty associated with human error.
The statements of the author reflect only his personal opinions and do not necessarily reflect the opinions of any institution with whom he is affiliated.
The author has a contractual or other financial relationship with Carl Zeiss Meditec, Inc. and has received financial support.